
What is the Intercondylar eminence?
The intercondylar eminence can be defined as the central part of the intercondylar area. It is easy to identify the intercondylar eminence, as it is both narrow and raised. As for the intercondylar area, this actually represents the central part of the tibial plateau.

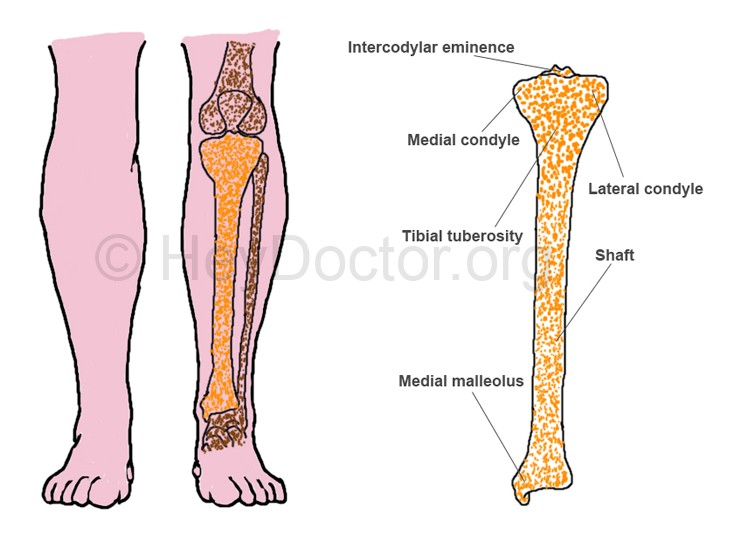
Intercondylar Eminence Picture (1) – Diagram showing the Intercondylar eminence, Medial condyle, Tibial tuberosity, Lateral condyle, Head, Tibia, Anterior crest, Fibula, Lateral malleolus and Medial malleolus.
It is a known fact that the intercondylar eminence is a structure of the tibia, being also presented as the tibial spine. As you will have the opportunity to read below, the intercondylar eminence is bordered by the articular facets of the proximal tibia. Prominent tubercles are located on either side of the intercondylar eminence. Apart from that, rough depressions are found in front and behind of the intercondylar eminence. These serve as point of insertion for the anterior cruciate ligament, the posterior cruciate ligament and the menisci.
The intercondylar eminence presents the medial and the lateral intercondylar tubercles. Both of them represent protrusions that occur at the upper extremity of the tibial bone.
Function of Intercondylar Eminence
Both the medial and the lateral intercondylar tubercles contribute to the delimitation of the intercondylar eminence. Thanks to its position, the intercondylar eminence actually divides the intercondylar area into a posterior and anterior surface.
Intercondylar Eminence Picture 2
Pathology
The intercondylar eminence is often involved in fractures. These fractures were described for the first time in 1875, by Poncet. Children and adolescents are often at risk of suffering from intercondylar eminence fractures; these often occur after small injuries and they are very-well treated through the procedure of anatomic reduction. Adults can suffer from this type of fracture as well but the damage is often more extensive (involving the knee) and the anatomic reduction does not guarantee the best outcome.
At the moment, the best intervention for the intercondylar eminence fractures is the arthroscopic approach. In the future, doctors are hoping to use bioabsorbable implants and thus eliminate the more invasive surgical interventions.
There are three main types of intercondylar eminence fractures, meaning: type 1 (the avulsed fragment presents minimal displacement and the bony apposition remains excellent), type 2 (anterior displacement of the bone – partial; leads to the appearance of a characteristic aspect on the X-ray – beak-like deformity) and type 3 (complete separation of bone fragment; no bony apposition). More recently, a type 4 has been proposed, being characterized by the comminuted avulsed fragment and associated displacement.
The laxity of the anterior cruciate ligament might be involved as a precipitating factor in the intercondylar eminence fractures. It is possible that the fracture can involve the tibial plateau as well. Some patients also present associated injuries to the meniscus or the other ligaments (for example, a tear in the medial collateral ligament). These injuries are often diagnosed in adults and they are often produced in motor vehicle accidents. In children, the intercondylar eminence fractures are caused by bicycle accidents (immature skeleton).
The incidence of the intercondylar eminence fractures has increased in the past few years. As more and more teenagers start to practice different sporting activities at an early age, the risk for such kind of fractures increases. The arthroscopic reduction, along with the fixation of the displaced bone fragment, remains the main choice of treatment.
As for the actual symptoms, most patients suffer from knee pain and they are unable to bear weight on the affected leg. If hemarthrosis has occurred as a result of the fracture, effusion might also be present. Because of the pain, the tendency is to keep the knee in a fixed position. However, the administration of analgesics allows the patient to resume the normal range of motion. Some patients might present the locked knee syndrome, which is highly suggestive of additional knee pathology.
The diagnosis of the intercondylar eminence fracture is made based upon the physical examination of the patient but also with the help of imaging studies. X-rays are often sufficient for the diagnosis, with the lateral view providing the most useful information. CT scans are generally recommended in adults who present additional pathologies, so as to ascertain the integrity of the tibial plateau. The MRI is recommended only in the situation that the patient also presents ligamentous or meniscal pathology.
These are the methods used for the treatment of intercondylar eminence fractures: arthroscopic reduction, open reduction and internal fixation and hemarthrosis aspiration, followed by casting (type 1 fracture).
Physical therapy is essential during the post-operative period. The physical therapist will design a program that is destined to help the patient recover as fast and as best as it is possible. The physical therapy program desires to allow the joint to regain the normal range of motion and also to increase the strength of the muscles in the area. After a few days, the patient is allowed once more to bear weight and the practice of gait (with or without assistive devices) is started.

